
Treatment Investment:
Building a True Continuum of Care for the Severely Mentally Ill and Addicted



The recent White House Executive Order “Ending Crime and Disorder on America’s Streets” presents a unique opportunity to undo the harms that were caused by the reckless deinstitutionalization of the mentally ill.1 The Executive Order takes aim at decades of failed policies that have allowed millions of Americans to suffer due to untreated mental illness and addiction. President Trump’s call to restore involuntary treatment for individuals who are too unwell to seek it themselves will reopen doors to institutions that were once devoted to saving lives, but have long languished under the poisonous idealism of the anti-institutional crusade.
State governments should answer the president’s call and begin a generational investment in treatment and services for people with severe mental illness and addiction. The policy changes asked of states are wide in scope, spanning healthcare, legal, and criminal justice systems. The cost to implement these changes to state general funds will be high, but the costs of failing to enact them will be paid in the lives of the most vulnerable members of our communities. The moral requirement to act and invest in treatment has never been more urgent.
Expanding Treatment
Part 1: Improved crisis intervention and emergency services.
Part 2: Expand inpatient psychiatric care.
Part 4: Increase utilization of Certified Community Behavioral Health Clinics (CCBHC).
Part 5: Expand residential treatment options, including housing with integrated treatment.
Part 6: Adapt legal standards for involuntary treatment to better meet the needs of the community.
a. Redefine the legal definition of “dangerousness”.
b. Expand the use of civil commitment laws.
c. Increase options for providing shelter that can be paired with behavioral health treatment.
d. Combine mental health courts and drug courts under a unified system of therapeutic justice.
e. Increase the use of Assisted Outpatient Treatment (AOT) and Assertive Community Treatment (ACT).
f. Increase the use of Forensic Assertive Community Treatment (FACT).
Part 1: Improved Crisis Intervention and Emergency Services

A mentally ill homeless individual’s first interaction with the legal system is often through law enforcement, resulting from a disturbance of social order or erratic behavior.2–3 In 1988, as a response to the rising interactions between the police and the mentally ill, the Memphis Police Department created the first Crisis Intervention Team, in partnership with the National Alliance for the Mentally Ill (NAMI), which has become the model for law enforcement responses to the mentally ill in crisis.4 However, due to inaccurate perceptions of police use-of-force, especially with the mentally ill, what started as a collaborative model between law enforcement and mental health practitioners has devolved into police agencies often working in isolation to address this growing crisis.5 A truly collaborative, co-responder model presents the best practice in addressing these crises by utilizing trained mental health providers to provide immediate evaluation and referral services in conjunction with a law enforcement partner.6 This model has been shown to increase efficiency through reduced calls for service while improving access to care.7–8 Further, cost savings due to reduced arrest and incarceration and increased community trust have also been found to be benefits of the co-responder model.9 The use of officers trained in crisis intervention and partnered with a mental health or addiction expert is an invaluable response resource that the local CCBHC can facilitate.
The CCBHC, discussed in more detail in part four, is key to effective co-response crisis intervention as they are required to provide 24/7 comprehensive crisis services, making them the natural partner for law enforcement.10 Through mobile team service and increased access to brick-and-mortar facilities to provide mental health and/or substance abuse treatment, the CCBHCs establish a continuum of community-based care. These services assure the best possible approach to care while reducing pressure on law enforcement, emergency departments, and hospitals to accommodate people experiencing a mental health emergency. The Substance Abuse and Mental Health Services Administration (SAMHSA) has published a manual of best practices in crisis intervention, highlighting mobile crisis response teams and stabilization services as core services, and these approaches should be implemented nationwide.11
Part 2: Expand inpatient psychiatric care
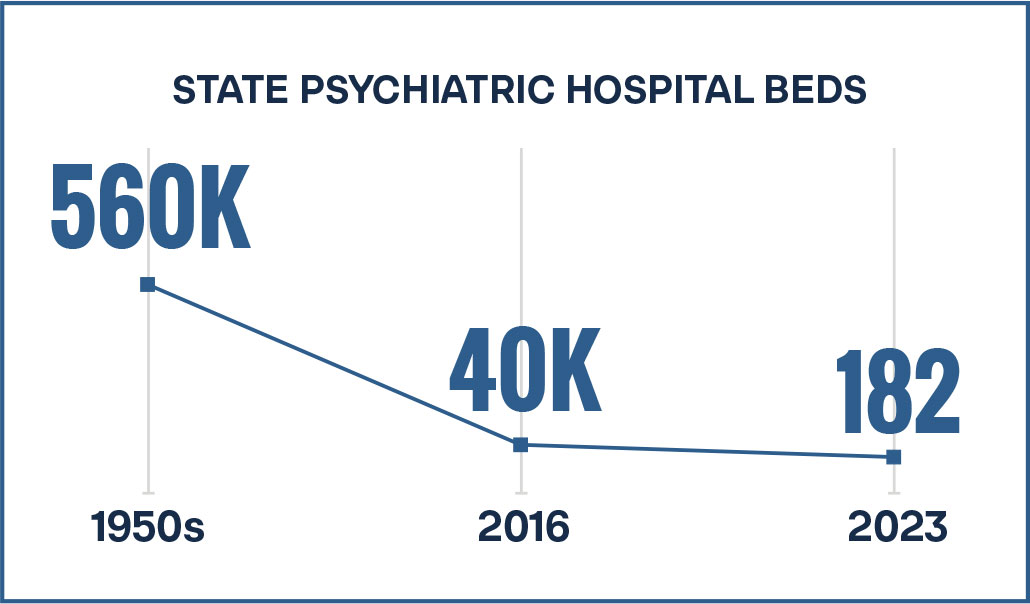
The purpose of a state psychiatric hospital is to provide around-the-clock supervised care to those suffering from severe mental illness or co-occurring disorders.12 The deinstitutionalization movement has resulted in a 93 percent reduction in state psychiatric hospital beds since its peak of 560,000 in the 1950s. As of 2016, there were fewer than 40,000 beds remaining.13 As of 2023, there were only 182 state-funded psychiatric hospitals.14 A 46-state review found the median number of hospital facilities per state stands at a meager two, 16 states had only one, and 80 percent of states reported a severe shortage of psychiatric beds.15 This phenomenon has not occurred by chance, as legislative barriers to inpatient psychiatric care persist. For example, Medicare only covers 190 days of residential psychiatric care over an individual’s lifetime.16 Medicaid Institutions for Mental Diseases (IMD) exclusions only allow payment for facilities with fewer than 16 beds.17 This is especially problematic given the current estimate of 15.4 million people in the United States who are battling a severe mental illness.18
Instead, due to the extreme shortage in psychiatric hospital beds, the severely mentally ill are being pushed into the streets, jails, prisons, and hospitals.19 While acknowledging that many with severe mental illness and addiction can live safely in the community, SAMHSA also recognizes the need to study how many of the 15.4 million are too mentally ill to be safely left in the community without 24/7 inpatient care.20 The American Hospital Association also recognizes the national crisis of too few psychiatric hospital beds, as the severely mentally ill tend to impact the nation’s hospitals in orders of magnitude greater than the jails, prisons, and homeless populations.21 Again, this is not by chance, as once a person hits their lifetime 190-day limit, their remaining options are limited to general hospital services.22 States need to increase the number of state psychiatric beds to at least a minimum number necessary to serve their severely mentally ill population. The Treatment Advocacy Center estimates that between 40 and 60 beds per 100,000 individuals are needed for the severely mentally ill who cannot live in the community. Current estimates show 11.7 beds per 100,000 individuals.23 To accomplish this, there are IMD Section 1115 demonstration waivers that states can apply for that allow for funding, but that is still a cumbersome process.24 Another alternative that states can use is the proceeds from opioid settlements, which can be used for co-occurring mental health and substance-use disorders.
Opioid settlement funds are the result of litigation that began in the late 2010s, culminating in large-scale agreements by 2021.25 State and local governments, alongside tribal entities, pursued claims against major pharmaceutical manufacturers and distributors, alleging aggressive opioid marketing practices and oversupply that fueled the addiction crisis.26 The resulting settlements, exceeding $50 billion, are to be disbursed over nearly two decades and represent one of the largest public health financial settlements in U.S. history. While these funds are designated for opioid abatement, states retain broad discretion in how to deploy them, creating a rare opportunity to invest in long-neglected behavioral health infrastructure, including expanded inpatient capacity for individuals with severe mental illness (SMI).
The following table displays cumulative and projected opioid settlement payouts to state and local governments, as compiled by KFF Health News using data from BrownGreer (court-appointed administrator of national opioid settlements).

As states are already receiving these funds, it presents as a more expedient funding stream than a waiver from the Institute of Mental Disease (IMD) or waiting for Congress to undo the discriminatory nature of the IMD exclusion through legislation.
Part 3: Encourage states to take advantage of Center for Medicare and Medicaid Services flexibilities on the Institutions for Mental Diseases exclusion
The Institute of Mental Disease (IMD) restrictions, produced by the legislature, have placed an unnecessary barrier to the treatment of mental illness and substance addiction.27 These restrictions on the use of Medicaid funding to support mental health care delivered in IMDs to those aged 21-64 date to the inception of Medicaid and reflect Congress’s unwillingness to fund large institutions to which people with SMI might be relegated for extended periods.28 Moreover, it displays a misunderstanding of the asylums of the early 1900s without understanding their purpose or successes.29 In the ensuing years, however, there has been recognition that inpatient mental health care is a vital resource for recovery and safety issues and for addressing severe mental illnesses and severe chronic addiction.30 Several pieces of legislation are now in place that make it possible for states to modify the IMD exclusion so that facilities principally serving those with severe mental illness can receive reimbursement for short-term treatment in these facilities.31 Further, in response to the opioid epidemic, Medicaid released new guidance to the states so that they could apply for an 1115 waiver to lift the IMD exclusion for the purpose of providing evidence-based treatment for opioid use disorder (OUD).32
The 1115 waiver can also include therapeutic residential treatment facilities for other drug-use disorders.33 Thirty-eight states have received 1115 waivers, and three states have applications pending specifically for SUD.34 Similarly, for severe mental illness, the 21st Century Cures Act permits states to apply for 1115 waivers for brief treatment in IMDs for adults with SMI and children with severe emotional disturbances. To date, 17 states have been granted these waivers, with applications from nine states pending. In addition, Medicaid Managed Care plans are permitted to pay for treatment of mental disorders in those aged 21-64 who are admitted to IMDs.35 This policy, first released in 2006, was codified into law through the 2018 Substance Use Prevention that Promotes Opioid Recovery and Treatment for Patients and Communities Act (SUPPORT Act P.L. 11-271) and provides Medicaid reimbursement for inpatient care for up to 15 days in the billing month. Further, Section 5052 of the SUPPORT Act added a new state plan option under SSA 1519 waivers.36–37 This option provides Medicaid coverage for enrollees aged 21-64 with at least one SUD for up to 30 days during a 12-month period. These IMDs must offer at least two FDA-approved medication-assisted treatments, and states must maintain outpatient SUD treatment efforts in their communities.38 States should be encouraged to review and utilize the above resources to improve mental health and substance abuse treatment services for their most vulnerable and severely ill.
A review and reconsideration of IMD exclusions by Congress is needed to facilitate a statutory change that lifts the IMD exclusion for state hospital beds. However, while Executive Order 14321, “Ending Crime and Disorder on America’s Streets,” does not explicitly address IMD exclusions, states should capitalize on the use of 1115 waivers to address the severely mentally ill and substance-use disorder population. Additionally, while we expect the number of civil commitments to be low, relative to the general population, those who are unresponsive to treatment through Assisted Outpatient Treatment (AOT) or Assertive Community Treatment (ACT) will need to be able to reside in a state hospital where they can be treated in a safe environment.39
Part 4: Increase utilization of the Certified Community Behavioral Health Clinic (CCBHC)
CCBHCs were created as part of the 2014 Protecting Access to Medicare Act to enhance and expedite comprehensive, coordinated access to mental health care and substance abuse treatment.40–41 By 2015, SAMHSA, working in partnership with CMS, awarded planning grants to 24 states to prepare for the Section 223 Medicaid CCBHC demonstration, which started in 2017 with eight states.42 Once the demonstration project funded by CMS began in 2017, there was further expansion to single sites in 2018 through the SAMHSA/CCBHC discretionary grant program, with funding to 64 providers that utilized the CCBHC model and provided the required behavioral health services.43 The CCBHC program moved toward program stability from 2019 to 2024 because of the proof of concept. In 2022, Congress passed the Safer Communities Act, which permanently embedded CCBHCs in statute with funding to expand to all states and the District of Columbia over time.44 In 2023, Congress awarded another $385 million for the expansion grant program after awarding $315 million in 2022 for the same purpose.45
CCBHCs are required to offer an array of behavioral health services. These include specifically:46
- Crisis services: mobile as well as freestanding facilities
- Screening, assessment, diagnosis, and risk assessment
- Treatment planning
- Outpatient mental health and substance use services
- Targeted case management
- Community-based mental health care for veterans
- Psychiatric rehabilitation services, including Assertive Community Treatment (ACT) and Assisted Outpatient Treatment (AOT)
The CCBHCs have proven to be effective in achieving outcomes. Eighty percent of them provide Medication for Addiction Treatment (MAT) for substance addiction, as opposed to the 64 percent nationwide in non-CCBHC settings, which is much more effective in managing withdrawal and addiction to opioids or alcohol.47 As related to making the streets safer for these individuals, those receiving CCBHC services experience a 72 percent reduction in hospital emergency room visits, 60.3 percent less time in jail, and a 40.7 percent decrease in homelessness, all of which is a focus of Executive Order 14321.48 Further, there is a substantially positive impact on care coordination for people who use the CCBHCs.49 With expanded access to care, and despite initial start-up costs, long-term cost benefit analysis shows a reduction in overall costs when reduced jail and hospital stays are considered.50 Finally, from an outcomes perspective, the CCBHCs are mandated to use data-driven accountability through comprehensive, transparent outcomes reporting.51
Expanding the CCBHC footprint will reduce jail populations, homeless populations, and emergency department visits, but it can be taken further. First, states should consider expanding CCBHC-provided care into the domestic violence shelters, which can provide the same access to treatment and support to victims of domestic violence, for which the Department of Justice has several grant programs. Second, the CCBHC should be used in a fully integrated co-responder model with law enforcement that supplants the current crisis intervention team (CIT) model used in policing. As noted, the co-responder model is the most effective evidence-based practice in addressing the risk and needs of the mentally ill and providing access to community-based services, given law enforcement’s first responder status.52 As the CCBHCs are already legislatively required to provide 24/7 access to mental health and substance abuse treatment, embedding these case managers with law enforcement presents a natural progression of CCBHC services while providing needed transparency to law enforcement to mitigate negative police interactions.53 Third, CCBHCs can be utilized in jail and prison settings through correctional-facility-based competency restoration programs. This provides newly released inmates a continuum of care that addresses mental illness and substance abuse needs, with the strong potential of reducing recidivism, and these correctional-facility-based services can be paid for using Mental Health Block Grant funds. This continuum of care for released inmates with severe mental illnesses can be readily achieved using AOT or FACT, which are programs overseen by CCBHCs in collaboration with civil and criminal courts.
Correctional-facility-based competency restoration is essential to restoring an offender’s competency to stand trial or determining whether the condition affecting competency is permanent and untreatable. Usually, competency restoration occurs in state hospitals, which puts an unnecessary additional burden on a medical system that is already inundated with severely mentally ill patients.54 As a result, the wait time for a hospital bed for competency restoration has resulted in a multitude of lawsuits due to Eighth Amendment violations based on deliberate indifference.55 Medicaid can be used for inmates who have been admitted to a hospital, but it cannot be used to provide treatment for inmates who are not hospitalized (i.e., in jail settings).56 Subsequently, CCBHCs have begun to find alternative funding sources to provide correctional-facility-based competency restoration before, during, and after a prison sentence.57 Interestingly, this is a less restrictive environment than the forensic hospital bed setting, and the program has been found to be very successful. One study found that 40 percent of those in a correctional-facility-based competency restoration program were restored to competency, 31 percent were diverted out of the criminal justice system, and 29 percent were referred to a more intensive program, due mainly to the jail’s policy on no use of involuntary medications.58–59 Using the CCBHCs to provide correctional-facility-based competency services reduces the negative financial impacts to the hospital and criminal justice systems and provides a continuum of care from a custodial to a community setting within one entity. This prevents the potential for individuals with severe mental illness and criminal histories from being “lost” for psychiatric and medical follow-up.
Part 5: Expand residential treatment options, including housing with integrated treatment
Addressing a problem of the magnitude of homelessness and mental illness requires an intensive and multifaceted approach that brings resources together from the outset to assist some of our most vulnerable and ill citizens. It is worth noting that, according to the National Alliance to End Homelessness, the “Housing First” model, which has been in place for nearly three decades, calls for:60
…a homeless assistance approach that prioritizes providing permanent housing to people experiencing homelessness, thus ending their homelessness and serving as a platform from which they can pursue personal goals and improve their quality of life. This approach is guided by the belief that people need basic necessities like food and a place to live before attending to anything less critical, such as getting a job, budgeting properly, or attending to substance use issues.
This approach is flatly wrong and does nothing to address the 25-30 percent of the more than 700,000 unsheltered homeless who have a severe mental illness, or the 75 percent who have a co-occurring substance abuse.61–62 The Housing First approach indicates that they see such issues as superfluous to obtaining housing, which has failed spectacularly.63 This program requires the person to agree voluntarily to treatment of their mental disorders and addictions; however, the reality is that the most severely mentally ill and substance-addicted do not think they have a problem and/or have no interest in obtaining treatment.64 These individuals will often require civil commitment to compel treatment. This is especially important for those who have histories of violent or destructive behavior toward themselves, others, or property. Therefore, civil commitment laws must be utilized at higher rates to compel treatment, as this will be necessary for positive outcomes and successful community placement for such individuals.65
Comprehensive, community-based treatment can now be addressed through partnerships with local CCBHCs that are structured to provide care for complex mental health and substance abuse treatment. Any housing services must be linked to mental health and/or substance abuse treatment for a person to become accountable and responsible for their own lives and maintain themselves in their communities. The resources necessary to provide a comprehensive system of behavioral health-supported housing services focused in communities already exist through the CCBHCs utilizing AOT (in-house and mobile services), ACT (mobile care teams), and FACT (for the criminally involved), and include integrated healthcare, case management, multidisciplinary treatment plans that provide whole person-centered care and connection to community services that help to integrate the individual into community life, when appropriate. These must be linked to any government-funded housing support in communities to fully support the recovery and successful community integration of those who had previously gone untreated for their health and severe mental illness conditions, as well as those who are homeless and chronically unsheltered living on American streets. Further, CCBHC reimbursements should be structured to penalize failure to continue necessary treatment and failure to renew civil commitment without discussing with the court mental health providers (which should include a prescriber of psychotropic medications and modification of a court-approved treatment plan.
Addressing severe mental illness requires a continuum from confinement to community-based treatment. While the courts have mandated treatment in the least restrictive setting possible, based on the individual’s diagnosis and needs, this does not preclude the need for secure, permanent residential treatment, or a continuum of appropriate services where people can live safely in the community. The ability to civilly commit needs to be expanded based on the widely accepted concept of grave disability, to include drug and alcohol addiction, and the inability to care for oneself.66
The range of options for housing those who have been civilly committed to those who can live safely in the community requires facility-based solutions, including around-the-clock onsite behavioral health staff for supervision. For those who are committed, the federal government already has a model of special housing for the sexually violent predator (SVP) and criminally involved SMI populations within the Bureau of Prisons.67 Assisted Outpatient Treatment and FACT models are necessary for those who are civilly committed or criminally involved and can be augmented with housing options, when needed. HUD funding can be used for these housing options through its Section 811 Supported Housing Program, and Medicaid can cover necessary clinical services.
Medicaid rehabilitative services offer states the ability to provide a wide range of community-based services to adults with severe mental illness through coverage described in statute (§1905(a)(13) of the Social Security Act; 42 CFR 440.130(d)). These services can range from clinic services to clubhouse-type psychosocial rehabilitation services. Individual states decide what their mental health services will include, and the federal government can assist in that decision-making process by promulgating evidence-based practices.68 In addition, HUD funding can address both housing and mental health needs, while Medicaid pays for community and home-based mental health services. Many states use home and community-based service waivers (HBCS waivers) to pay for support services to individuals with disabilities, including those with mental health conditions. Similarly, home health services can include case management, individual, group, or family therapy, medication management, and other intensive services that may be necessary to address severe mental illness needs.
A further facet of community-based psychosocial support is the clubhouse model. This model fosters recovery and stability through socialization, vocational assistance, and educational opportunities, along with the aforementioned treatment plans.69 Engaging this population through utilization of these resources has been shown to improve quality of life and relationships, reduce hospitalizations, increase the likelihood of employment, and lower Medicaid costs for participants.70
Part 6: Adapt legal standards for involuntary treatment to better meet the needs of the community:
a. Redefine “dangerousness”
The definition of “dangerousness” as it relates to mental health and criminal justice is often ambiguous and disparately applied across the states. In fact, the Treatment Advocacy Center has found that the practical application of the dangerousness standard has resulted in 50 separate definitions, each with different standards and criteria for involuntary commitment based on divergent legal and clinical definitions.71 The result is that the courts often rely on the simplest definition: that the person must be an imminent danger to themself or others. However, using this narrow definition severely limits the preventive capabilities of the courts through diversion programs because the individual is required to have committed or was planning to commit a harmful act against themselves or someone else. Further, this narrow definition of dangerousness does not give any credence to the clinical acknowledgement of a “downward spiral” that represents the self-perpetuating degradation of a person’s mental state due to the course of illness, stress, lifestyle, etc., that leads to more intense responses (i.e., psychotic episodes) resulting in a full-blown psychotic break.72–73
Conversely, certain states, such as North Carolina, have taken a more expansive view of dangerousness for both danger to self and others. Specifically, danger to self within the North Carolina Statute includes:
Dangerous to Self
Within the relevant past, the individual has done any of the following:
- The individual has acted in such a way as to show all of the following:
I. The individual would be unable, without care, supervision, and the continued assistance of others not otherwise available, to exercise self-control, judgment, and discretion in the conduct of the individual’s daily responsibilities and social relations, or to satisfy the individual’s need for nourishment, personal or medical care, shelter, or self-protection and safety.
II. There is a reasonable probability of the individual’s suffering serious physical debilitation within the near future unless adequate treatment is given pursuant to this Chapter. A showing of behavior that is grossly irrational, of actions that the individual is unable to control, of behavior that is grossly inappropriate to the situation, or of other evidence of severely impaired insight and judgment shall create a prima facie inference that the individual is unable to care for himself or herself.
- The individual has attempted suicide or threatened suicide and that there is a reasonable probability of suicide unless adequate treatment is given pursuant to this Chapter.
- The individual has mutilated himself or herself or has attempted to mutilate himself or herself and that there is a reasonable probability of serious self-mutilation unless adequate treatment is given pursuant to this Chapter.
Previous episodes of dangerousness to self, when applicable, may be considered when determining reasonable probability of physical debilitation, suicide, or self-mutilation. (N.C. GEN. STAT. § 122C-3(11).74
This expanded definition of danger to self provides a realistic look at the probability that someone suffering from severe mental illness will ultimately experience a worsening physical condition due to their mental state without treatment. As such, the ability to provide compulsory mental health treatment, both in inpatient and outpatient settings, depending on the level of acute severity, is justified. Minnesota, which received the highest grade rating on commitment laws from the Treatment Advocacy Center, is more succinct in its definition of dangerousness.75 According to Minnesota Statute §253B.09, the court may involuntarily commit a person if the state proves by clear and convincing evidence that s/he is mentally ill, developmentally disabled, or chemically dependent.76–77 Minnesota Statute §253B.02 defines mentally ill as:
- Any person who has an organic disorder of the brain or a substantial psychiatric disorder of thought, mood, perception, orientation, or memory;
- Said disorder grossly impairs judgment, behavior, capacity to recognize reality, or to reason or understand; as a result, poses a substantial likelihood of physical harm to self or others. Minnesota’s definition for compulsory treatment relies on “the least restrictive treatment program or alternative programs which can meet the patient’s treatment needs consistent with section 253B.03, subdivision 7”, and consistent with the Olmstead v. L.C. (1999) decision.78–79 Beneficially, this definition is based on a patient’s right to care rather than on a right to refuse care model that has been widely misrepresented by behavioral health advocates. This is an important distinction given the probability that an individual struggling with addiction and/or SMI may not be of sound mind and body to make a rational decision regarding care.80 Regardless, the least restrictive setting standard is often interpreted to mean the right to refuse care. The right to refuse care has, unfortunately, left individuals in crisis untreated due to incorrectly perceived violations of their civil liberties. This situation has arisen from inaccurate interpretations of the National Institute of Health’s definition of the right to refuse, which is based on the capacity and competence for one to understand their basic need for treatment.81
The assessment of an individual’s capacity to understand treatment options and criminal proceedings is integral to the definition of dangerousness and civil commitment, as shown by the previously discussed North Carolina standards for commitment. Research has found that incapacity is common. Twenty-nine percent of those studied who had psychosis, symptom severity, and treatment refusal significantly correlated to incapacity.82 Given this, the right to treatment for those deemed dangerous, compulsory or not, should be part of a redefinition of dangerousness.
Specifically, dangerousness should be redefined as a threat of physical harm to self or others, or the probability that an individual will deteriorate physically and mentally to a point of imminent threat without treatment due to grave disability.
b. Expand the Use of Civil Commitment
States should expand involuntary civil commitment for treatment of mental disorders to include co-occurring “substance use disorder” (SUD) addiction treatment based on comorbidity research. Currently, the maximum amount of time that a person can be held on a psychiatric hold is 72 hours, though several states hold for longer.83 However, with involuntary substance abuse holds, the length of time is less defined, with states ranging from 60 days in Florida, to 90 days in South Carolina, and 270 days in Colorado with the option of recommitment if the initial involuntary commitment did not achieve the desired outcomes.84 Florida’s Marchman Act explains this expansion of involuntary holds for substance abuse because:
…of the impairment or disorder, he or she has lost the power of self-control with respect to substance abuse. AND
- Is in need of substance abuse services, and by reason of substance abuse impairment, the person’s judgment is so impaired that the person is incapable of appreciating the need for, and is unable to make a rational decision in regard to, substance abuse services. OR
- Without care or treatment, is likely to suffer from neglect or refuse to care for himself; and that such neglect or refusal poses a threat of substantial harm to himself or herself; and that it is not apparent that such harm may be avoided through help of family or friends, or there is substantial likelihood that the person has inflicted, attempted or threatened to inflict, or unless admitted, is likely to inflict, physical harm on himself or herself or another.85 The law acknowledges that someone under the influence of drugs or alcohol lacks the capacity or competence to make rational decisions, has lost self-control, and has a great potential for harm.86 Additionally, SAMHSA has reported that approximately 50 percent of those with mental illness struggle with addiction, and the percentages climb in populations with SMI.87 This begs the question of why reduced capacity and competence for someone with a history of substance abuse can be acknowledged and met with involuntary commitment for long periods, when they have the potential to get better, yet cannot do the same for the severely mentally ill with a chronic, relapsing illness for which there is no cure.
The percentage of the severely mentally ill that would need permanent involuntary commitment is relatively small, approximately 10 percent of the total mentally ill population.88 Yet, this population has been shown to have a disproportionate impact on the criminal justice and hospital systems, and comprises a significant proportion of the homeless population. Allowing for civil commitment based on a broader definition of dangerousness that accounts for diminished capacity and comprehension, similar to involuntary holds for substance abuse, with an expanded period of time, such as Florida’s Marchman Act 60-day hold, would allow greater opportunities for appropriate acute responses and for establishing treatment plans based on the high likelihood of co-occurring disorders.89
Expanding involuntary civil commitment to include those who lack capacity and comprehension to make informed decisions regarding their treatment needs due to SMI is essential in assessing and treating a population that disproportionately impacts multiple systems. Redefining dangerousness the severely mentally-ill allows patients to be assessed and provided treatment based on a right to treatment when the escalation of associated behaviors shows that there is a probability that the individual being treated will become an imminent threat to themself or others due to repeated and continuous inability to care for their self (e.g., mentally, physically, etc.), and violations of the social order (e.g., trespassing, and public disorder crimes). As the impact of the severely mentally ill on correctional facilities, hospitals, and homeless services has been discussed, the question then becomes where to house these individuals when they need compulsory residential treatment.
c. Options for Providing Shelter that can be Paired with Behavioral Health Treatment
There are reports that the federal government had 8,000 unused facilities across the country as of 2023.90 This number is down from the reported 77,000 in 2014, but still represents a significant opportunity to secure housing for the most severely mentally ill.91 Unfortunately, the federal bureaucracy has precluded this quick response approach, even in the wake of a 2016 law (the Federal Assets Sale and Transfer Act) stating that these facilities should be used to house the homeless.92–93 These facilities include hospitals and dorms, which provide a unique opportunity to enact a stepped approach to treatment for the severely mentally-ill. Yet, they sit vacant, paid for in countless lives lost among our nation’s forgotten homeless, addicted, and mentally ill.
An alternative approach is to utilize similar state-owned property. Unfortunately, unused real property at the state level is far more challenging to track as each state maintains its own databases with different standards, which may or may not be readily transparent. Given the direction of Section 3 (iv) of Executive Order 14321, which notes;
“…where necessary, adopt standards that address individuals who are a danger to themselves or others and suffer from serious mental illness or substance use disorder, or who are living on the streets and cannot care for themselves, through assisted outpatient treatment or by moving them into treatment centers or other appropriate facilities via civil commitment or other available means,”
The need to assess state-level real property assets is vital to compliance with the Executive Order.94 Federally, the Obama administration had an interactive map that showed the locations of all federally owned real property (Figure 1).95
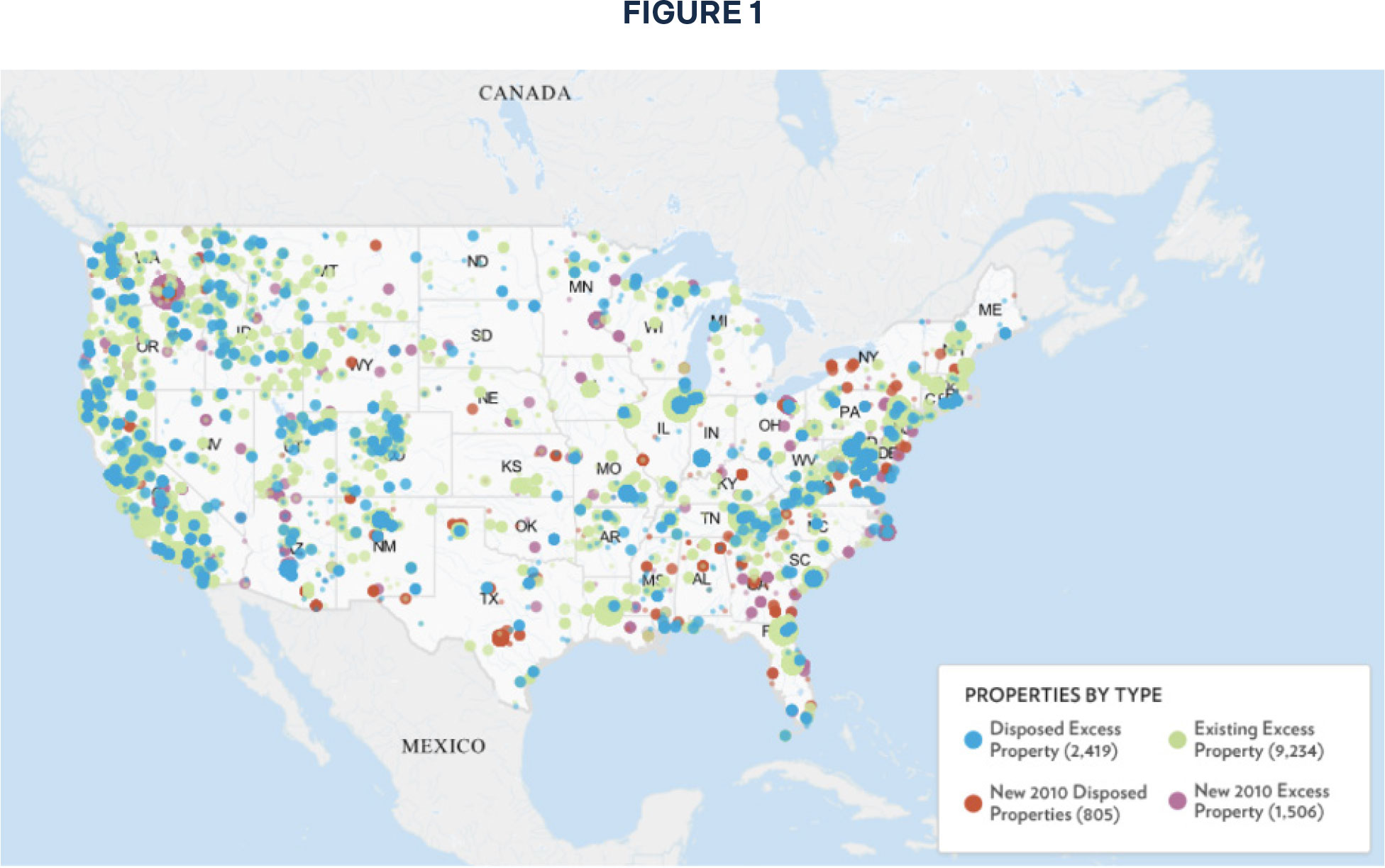
While this map is outdated, recent efforts under the Trump administration through the Department of Government Efficiency (DOGE) have added further federal buildings to the unused inventory through consolidation and reorganization.96 So, even if states do not have an accurate accounting for their unused real property inventory, federal properties remain a viable option given that, according to the database, there are more than 2,700 facilities nationwide that can be readily converted to serve the 10 percent of all severely mentally ill that need compulsory residential treatment.97 These facilities include unused schools, hospitals, correctional facilities, family housing, offices, and more.
d. Combine Mental Health Courts and Drug Courts under a unified system of therapeutic justice.
The drug court movement started in 1989 and has grown to more than 4,000 drug courts nationwide.98 It is believed that this number includes driving under the influence, or “DUI” , courts and newly formed opioid courts.99 These diversion court settings offer individualized treatment plans in lieu of incarceration or other punishments that can last months or years, depending on the individual’s case and criminal history. Drug courts report a 35-40 percent reduction in recidivism with a cost savings of over $6,700 per offender in reduced rearrest alone.100 The drug court program for adults was so successful that it was expanded to the juvenile courts in 1995 because of the focus on treatment of a chronic condition that impacts behavior and impulse control, as opposed to the punitive ideology in regular courts.101
Similarly, the mental health court program grew from four courts in 1997 to more than 300 in 2020 with a similar focus on therapeutic jurisprudence over punishment for those diagnosed with a severe mental illness.102 Significantly, due to the complex nature of diagnosing and treating the severely mentally ill, the mental health courts rely on a team of experts to assign, treat, and monitor individuals in the mental health court system. However, it is the very complexity of treatment that has prevented the mental health court system from growing to the same extent as the drug courts. As a derived subset of drug courts, mental health courts also treat co-occurring substance abuse, but that relationship is not reciprocal, meaning that drug courts do not typically also address underlying mental illness.103–104
The Council of Chief Justices and the Council of State Court Administrators passed a joint resolution in 2000 calling for the various specialized courts to combine into one “Problem Solving Court” model.105 Through combining drug and mental health courts, redundant government assets can be streamlined to offer faster, more effective, integrated, and holistic service delivery from the therapeutic court. While maps often show the statewide totals for therapeutic courts, these maps often look at adult drug, hybrid drug/ DUI, DUI/DWI, and opioid courts as separate entities across the country and often drive states to do the same.106
Notably, there is an acknowledgement of co-occurring disorders among adults with the growth of 44 adult co-occurring disorder courts due to the large body of empirical research on the impact and prevalence of co-occurring disorders in the prison population, as well as in law enforcement encounters, where 25 percent of officer-involved fatalities involve a mentally-ill suspect, and another 23 percent involve suspects with a history of substance abuse.107–108 While these two conditions are often treated as separate entities within the criminal justice system, they should not be. Conservative estimates find that almost half of individuals with severe mental illness also struggle with addiction.109 Instead of shuffling individuals from one court system to the next, combining drug and mental health courts has the potential to provide treatment options under one umbrella, much like the ACT model. Orange County, California has already moved toward this in an effort to improve service delivery and efficiency while reducing redundancy.110
e. Increase the Use of Assisted Outpatient Treatment (AOT) and Assertive Community Treatment (ACT)
Assisted Outpatient Treatment (AOT) is a civil court-ordered treatment program to assist non-compliant, severely mentally ill people in adhering to their treatment plan.111 The court order motivates high-risk individuals to adhere to treatment protocols through sanctions and rewards or be subject to involuntary commitment, and allows providers to focus on keeping a defendant in a court case engaged in their treatment. Similar to a guardian ad litem, mental health practitioners safeguard a mentally ill defendant’s due process rights while maintaining open lines of communication with the court. The civil court aspect is necessary for both the lower standard of proof with regard to preponderance of the evidence versus beyond a reasonable doubt, and the lack of threat of criminal proceedings and the potential for a conviction. This allows for greater flexibility in court proceedings and determinations without the potential for legislatively imposed sentencing guidelines that are present in the criminal justice system.
Assertive Community Treatment (ACT) is a team-based behavioral health model that brings mental health and substance abuse treatment directly into the community for individuals who cannot or will not attend medical appointments. ACT focuses on a smaller population than Assisted Outpatient Treatment (AOT): people with severe mental illness who are unable or unwilling to engage in traditional care settings. Unlike AOT, ACT is not court-ordered but provides intensive, individualized treatment plans tailored to each patient’s needs and capacity to participate. Together, AOT and ACT represent complementary approaches across the behavioral health care continuum.
f. Increase the use of Forensic Assertive Community Treatment
A further iteration of ACT is Forensic Assertive Community Treatment (FACT), which incorporates the criminal justice system, as opposed to the civil justice system.112 AOT and ACT involve at-risk populations not yet involved in the justice system, and with AOT still bringing about the weight of the court in civil commitment. FACT models invoke the weight of the criminal justice system with the potential for incarceration as well as involuntary commitment. For those who are in the justice system, FACT models can offer the potential for suspended criminal sentences and withheld adjudication for those who participate in and complete treatment.113 Much like CCBHCs, FACT programs have been shown to result in fewer days of incarceration and hospitalization with a return on investment of $1.50 for every dollar spent, representing cost savings to the taxpayer. FACT programs are a model representation of the mental health and criminal justice co-responder model.
Moving forward, FACT programs should be used for individuals with SMI or severe SUD/AUD who have become criminally involved and fall into specific categories. FACT is appropriate for those under court-ordered community supervision (probation), incarcerated and close to parole, or recently released from prison or a forensic hospital.114 Similarly, ACT should be the focus for those who have been deemed severely mentally ll with grave disability and/or dangerousness to self/others and non-compliant with treatment and are not criminally involved.
Summary
The purpose of this paper is to lay out a multi-pronged plan of action that states can follow to address problems of severe mental illness and severe substance abuse in compliance with Executive Order 14321. Given the high rates of severe mental illness and addiction in prisons, jails, emergency rooms, and homeless populations, it is imperative to address the treatment of these conditions, and to do this simultaneously.
The United States has reverted to old practices of casting the severely mentally ill and addicted into the streets without treatment under the ruse of protecting civil rights. Today, we have treatments and responses, but are relegated to outdated legislation that is hindering response and creating chaos in the streets. It is long past time to address these co-occurring issues. The solutions offered in this research include best practices and innovations in behavioral health and propose models for combining behavioral health, addiction, and housing resources that can be implemented to address the complex needs of this subpopulation while also increasing the quality of life for all living in communities affected by homelessness compounded by severe mental illness and deadly drug addiction.

Stay Informed
Sign up to receive updates about our fight for policies at the state level that restore liberty through transparency and accountability in American governance.