
Addressing Psychiatric Capacity through Trans-Institutionalization of Involuntarily Committed Sex Offenders

Introduction
Sex offenders constitute an exceptional category of individuals in American law and society. More so than other crimes, a conviction of a sexual offense carries extensive restrictions and supervision as part of state sex offender registries. These last far longer than probation, prison, parole, or other types of post-release supervision for different crimes. In 20 states, public policies go even further, permitting a civil commitment procedure for a subset of sex offenders deemed “sexually violent predators.”1 These laws allow for sex offenders who have a mental abnormality and a high-risk profile to be civilly committed to psychiatric institutions for treatment and the protection of the public.
Civil commitment of sex offenders is an essential tool of public safety. Still, it has created significant strain on a system that was designed for a different purpose: treatable psychiatric care. In part due to sexually violent predator laws, nearly all states face a shortage of psychiatric beds for patients civilly committed through other procedures. Instead of dismantling sexually violent predator laws, states should create distinct institutions that are better designed to handle this subpopulation of civilly committed patients. This approach would alleviate the pressure on psychiatric beds in state hospitals while also ensuring that the public safety benefits of civil commitment of dangerous sex offenders remain.
Involuntary Civil Commitment of Sex Offenders
The U.S. is unique in its policy of civilly committing some sex offenders to psychiatric institutions under distinct procedures from all other types of psychiatric commitment. This practice began in the early twentieth century as part of a movement to classify sex offenders, especially those who committed crimes against children, as “sexual psychopaths.”2 It was relatively unusual for child molesters to receive prison sentences until after the mid-twentieth century.3 Before then, child molesters most often received probation sentences, and some were committed to psychiatric institutions in connection with their offending patterns. The latter half of the twentieth century brought a dramatic shift in policy towards sex offenders, with increased reliance on long prison sentences and, for a few decades, little attention to obsolete or repealed sexual psychopath laws.4
Renewed interest in the civil commitment of sex offenders came towards the end of the twentieth century, with states adopting a new paradigm called “sexually violent predator” laws.5 These laws allow states to designate certain sex offenders as sexually violent predators, which became a special classification within the sex offender registry that has heightened community notification requirements and permits prosecutors to petition courts to civilly commit such offenders to psychiatric institutions under a lower standard than applies to the general population.6 Instead of requiring individuals to exhibit signs of severe mental illness and present an immediate danger to themselves or others as evaluated by a psychologist, sexually violent predators need only be shown to have a “mental abnormality,” a vague standard that falls outside of the Diagnostic and Statistical Manual of Mental Disorders (DSM) and essentially allows for confinement of sexual offenders who would otherwise not meet commitment criteria.7 Because the treatment of a mental condition is one of the justifications of civil commitment, sexually violent predator laws have a pretext of treatment. Miller (2010) points out that treatment is fairly limited in these facilities, and offenders have strong disincentives to participate in treatment or discuss their crimes or underlying sexual deviance.8 The result is that those committed tend to stay in psychiatric facilities for periods that may exceed their original prison sentence.9
Importantly, civil commitment of sexually violent predators need not happen in lieu of prison. Rather, prosecutors can petition for commitment upon release from prison or even after the individual is back in the community. These laws have been the subject of significant litigation, but ultimately, the U.S. Supreme Court ruled in Kansas v. Hendricks (1997) that they did not violate the Fourteenth Amendment’s protections of due process or against double jeopardy.10 By 2006, more than 4,500 individuals were committed under sexually violent predator laws nationwide.11

States with Sex Offender Commitment Laws
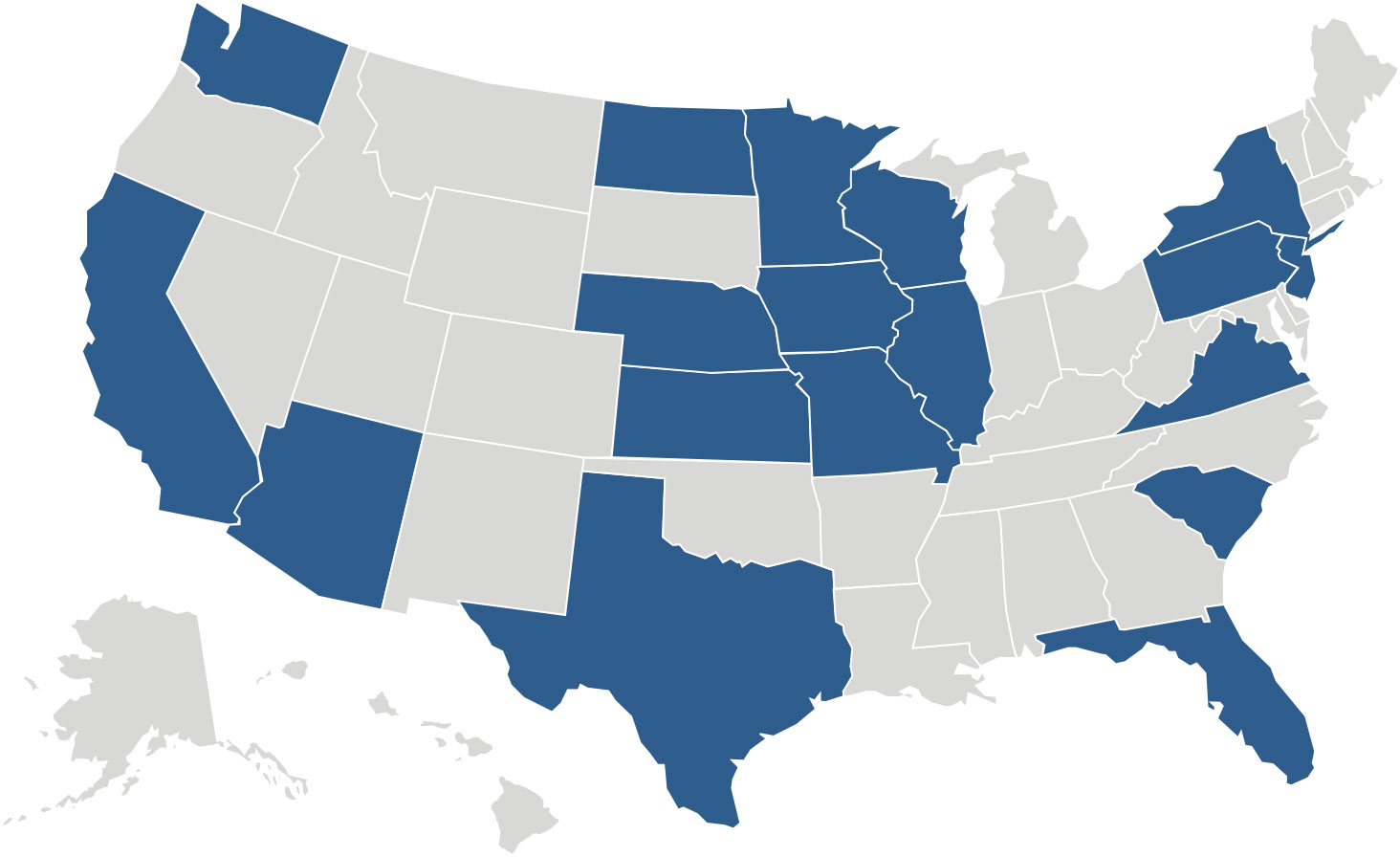
Twenty states have some version of a sexually violent predator law that permits the involuntary civil commitment of certain sex offenders. These states include Arizona, California, Florida, Illinois, Iowa, Kansas, Massachusetts, Minnesota, Missouri, Nebraska, New Jersey, New York, North Dakota, Pennsylvania, South Carolina, Texas, Virginia, Washington, and Wisconsin.12
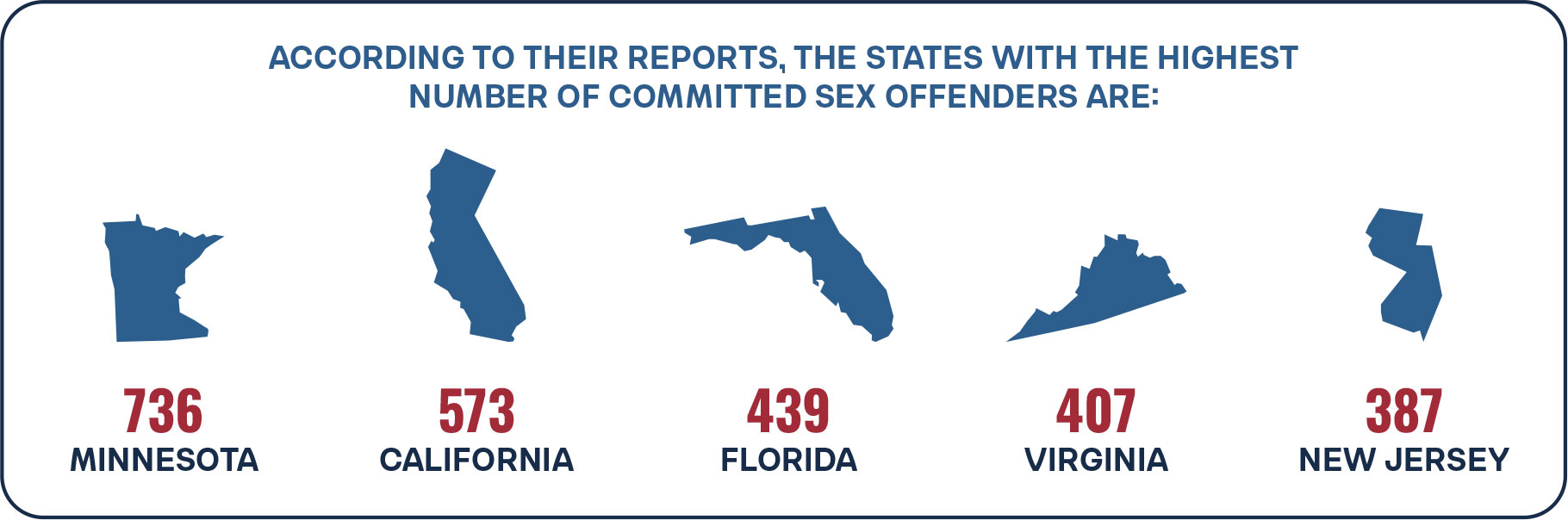
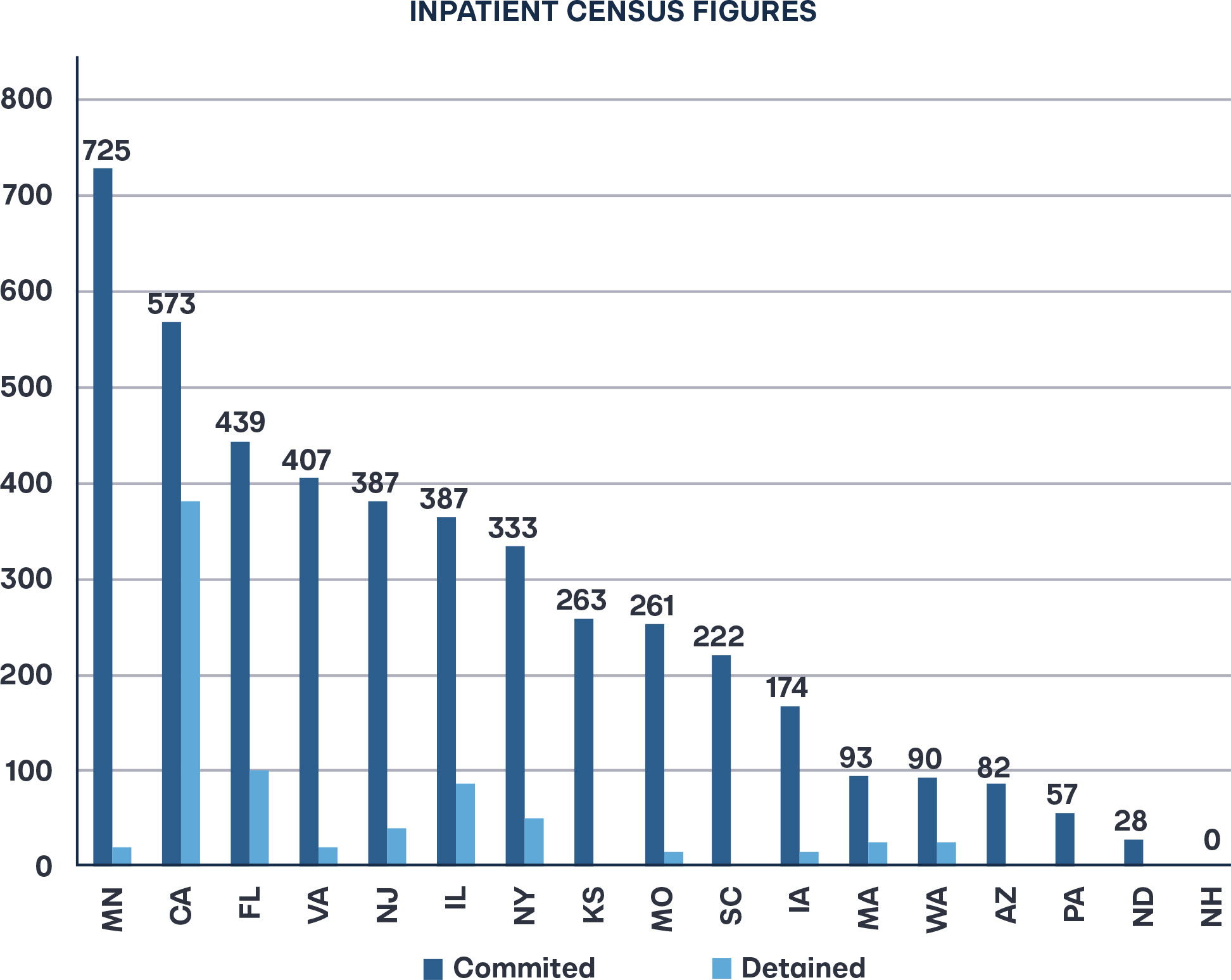
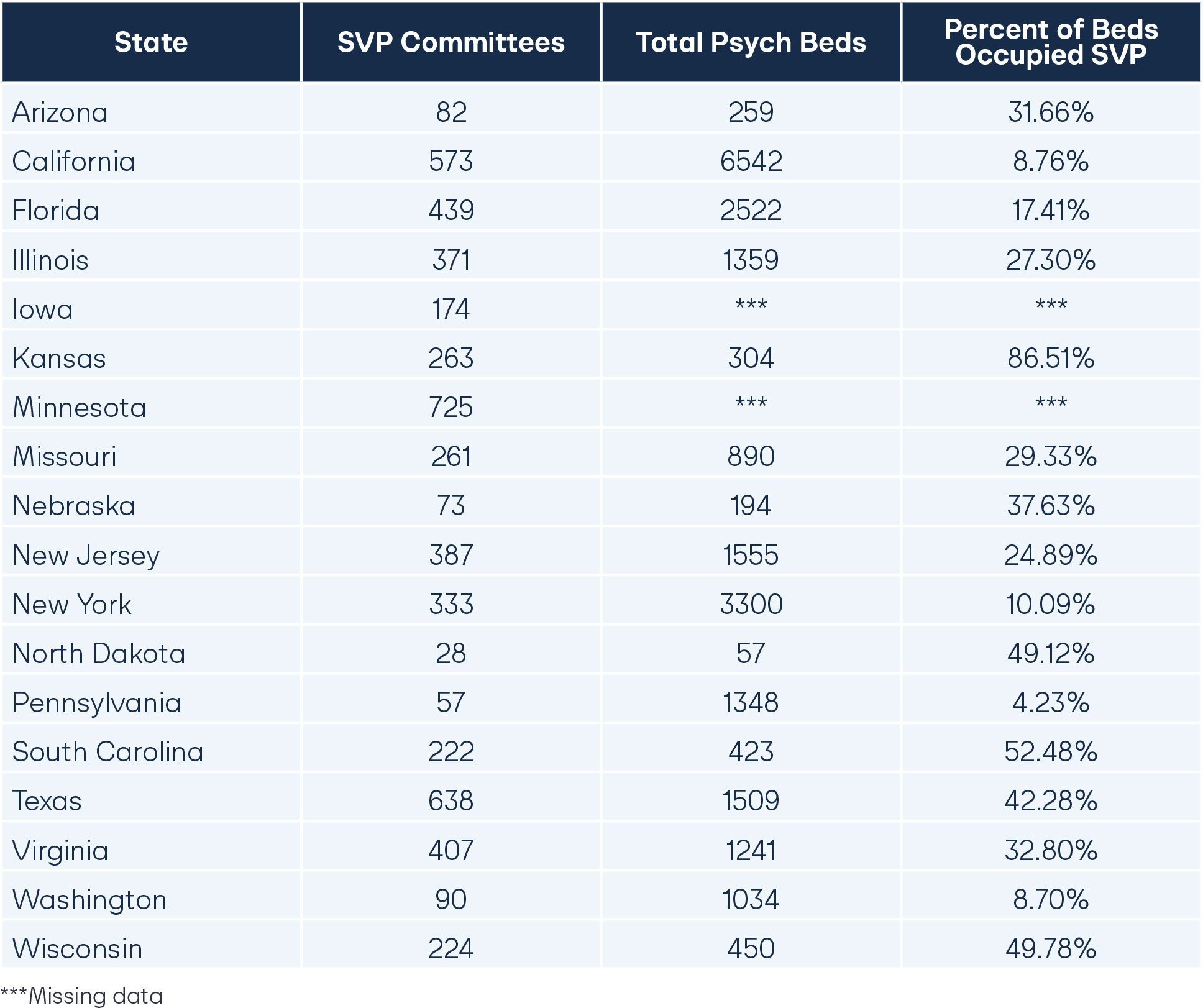
Research on sex offender civil commitment policies is relatively limited, and most states do not regularly publicize information about their civilly committed population. The Sex Offender Civil Commitment Program Network provides the most detailed information on these policies, and they conduct an annual census of the committed sex offender population in each state.13 According to their reports, the states with the highest number of committed sex offenders are Minnesota (736), California (573), Florida (439), Virginia (407), and New Jersey (387).14 The median number of committed offenders across states is 260 people. Across the 19 states that responded, the total committed population was 5,421.15 The vast majority of committed sex offenders, 78 percent, had victims who were children or had victimized both adults and children.16
Civilly committed sex offenders generally have high rates of active participation in treatment, ranging from 36 to 100 percent, with a median of 89.7 percent.17 Not all state psychiatric hospitals, however, provide treatment programs tailored to sex offenders.18 Nine states reported offering programs specifically for sex offenders, in addition to other programs related to psychiatric care.19 All states but one offer care primarily by psychiatrists, and nearly half also offer care by psychiatric nurse practitioners.20 The use of off-site community psychiatric services or telepsychiatry is relatively limited, but one state exclusively uses telepsychiatry.21 Thirteen states integrate psychotropic medication into their treatment of sex offenders, with about half of the committed sex offenders prescribed such medication, while medications intended to reduce sex drive are far less common.22 The median annual cost of treatment for involuntarily committed sex offenders is $139,000, with some programs as low as $93,000 and others as high as $294,000.23
Not all civilly committed sex offenders remain committed indefinitely. Courts regularly review commitment eligibility, and some states have created conditional release programs that function similarly to the criminal justice system’s parole system.24 Thirteen states—Arizona, California, Illinois, Iowa, Kansas, Massachusetts, Minnesota, New Jersey, New York, Pennsylvania, Virginia, Washington, and Wisconsin—have conditional release.25 The remaining states discharge with limited supervision. Not all states with conditional release use it widely, but approximately 1,315 people have been released under the program across all of these states.26 However, these releases come after years of inpatient treatment, ranging from an average of just under five years in New York to over a decade in California, Minnesota, and Wisconsin.27 The median time on conditional release across programs is 45 months.28
Transitional housing remains a significant challenge for this population, with it taking nine months on average to find an appropriate place to live after an individual is released.29 But those who do make it back into the community on conditional release after their intensive treatment fare quite well. Sex offenders conditionally released do appear to have better outcomes, avoiding re-offense at about twice the rate of those released without conditions.30

The Dangers Presented by Sex Offenders
Between 319,000 and 734,000 people in the U.S. indicated that they were victims of sex crimes annually between 2018 and 2022, according to the Bureau of Justice Statistics’ National Crime Victim Survey.31 Only one in five of these crimes was reported to the police each year, by far the lowest of any category of crime.32 Of those reported crimes, less than one-third led to an arrest by law enforcement.33
As such, the individuals who are convicted of sex crimes represent only a fraction—typically the most heinous fraction—of sexually violent criminals.
Yet, sex offenders do not typically serve very long prison sentences. The median time served in prison for people convicted of rape was just over 86 months, while the time served for people convicted of other forms of sexual assault was a mere 43 months.34 Most people convicted of sexual offenses at the state level were released far before the end of their full sentence. The Bureau of Justice Statistics found that the average percentage of a prison sentence served by a sex criminal was between 58 and 67 percent.35 Nearly two-thirds of convicted rapists served less than 10 years in prison, and nearly two-thirds of people convicted of other forms of sexual assault served less than five years.36
Approximately half of sex offenders released from prison recidivate within five years, the second lowest rate of any offense type, but still an alarmingly high rate considering the seriousness of the offenses.37 In fact, sex offenders have the lowest risk of committing any re-offense type except for public order offenses, for which they rank second lowest, and sexual assault, for which they reoffend at by far the highest rate.38 Sex offenders commit new sex crimes at between two and six times the rate of other types of offenders after release from prison.39
Sex offenders designated as sexually violent predators are typically considered the highest risk individuals, which is part of why they are subject to extraordinary policies like civil commitment.
Expanding Psychiatric Bed Capacity through Transfers of Sex Offenders
America is facing a catastrophic shortage of inpatient psychiatric beds.40 There are fewer than 40,000 beds available for inpatient psychiatric care nationwide, and Treatment Advocacy Center estimates that most states require between three and five times as many beds to care adequately for severe mental illness in the population.41 Yet, among the few psychiatric beds that do exist, roughly half are allocated to forensic, or criminal, patients.42 And in states with sexually violent predator laws, psychiatric beds must also be allocated to civilly committed sex offenders, many of whom have a much different psychiatric profile than other patients.43 Treatment of forensic and sex offender patients accounts for more than one-third of state psychiatric hospital expenditures nationwide.44
Expanding psychiatric bed capacity through investments in treatment and facilities is the most critical factor in addressing this crisis. But a substantial amount of bed capacity in some states could be unlocked through the redistribution of care for specialty populations like sex offenders.
Proposal: Transferring Civilly Committed Sex Offenders to Other Facilities
States that civilly commit sex offenders should create distinct facilities for this purpose. Such facilities would sensibly be located near professionals who work with incarcerated sex offenders, such as a prison or jail. Placement of a facility as part of a prison campus would allow for greater economies of scale, which would reduce challenges due to staffing and other resources. To utilize prison-adjacent facilities, however, a state must ensure that the institutional conditions of the civilly committed sex offenders are meaningfully different, non-punitive, and treatment-oriented compared to incarcerated sex offenders. These differentiating standards are essential. In People v. Feagley (1975), the Supreme Court of California found that civil commitment of a sex offender in an “institutional unit” on the grounds of a prison was unconstitutional because the facility in which the individual was confined could not be meaningfully distinguished from the incarceration of the general population, and there was no pretext of treatment. However, the U.S. Supreme Court held in Kansas v. Hendricks (1997) that the inability to offer treatment to sex offenders for underlying mental abnormalities does not undermine the state’s legitimate power to civilly commit them should they pose a danger to the public and possess such a mental abnormality. Crucially, a mental abnormality must still be present for a sex offender to be committed, but the spectrum of disorders covered by the “mental abnormality” standard is generally considered to be broader than a “mental illness.” Thus, a facility that meets these thresholds but is separate from a state psychiatric hospital could satisfy the legal requirements for civilly committed sex offenders, offer a viable option for transfer of custody, and alleviate high-demand psychiatric beds that would better serve individuals with serious mental illness who are not sexually violent predators.
Conclusion
Civil commitment is an essential tool on a continuum of responses to high-risk sex offenders. But such policies create significant strain on psychiatric bed resources due to the absence of distinct, sex offender-focused facilities that can better confine and care for this population. States should build such facilities, which need not be as expensive or robust as psychiatric hospitals and could be located near other institutions that offer some economies of scale. This would allow sex offenders to be transferred, freeing up high-demand inpatient psychiatric beds.

Stay Informed
Sign up to receive updates about our fight for policies at the state level that restore liberty through transparency and accountability in American governance.