
The History and Consequences of Deinstitutionalization



The Historical Emergence of “Mental Illness”
The early history of mental illness is rooted in ancient beliefs that a lack of spirituality was responsible for these conditions. Religious beliefs played a major role in attempting to care for and cure mental illness up to the 1300s, with the belief that if a person could become more spiritually and emotionally closer to God, they could then be cured.1 However, the majority of the mentally ill were not cared for by the Church. Rather, most mentally ill people were kept in family homes, but those whose behaviors were too difficult to manage or who had no family to try to care for them were cast out of homes and communities. They were forced to live in the countryside, struggling to survive—often unsuccessfully.
Major human catastrophes came to Europe in the 14th century. These included plague, highly lethal infectious diseases, and famine, which were attributed to evil spirits and demons. Those who were mentally ill and who experienced symptoms such as auditory and visual hallucinations or delusions were thought to be witches or sorcerers in collusion with the devil. Some were jailed, some were executed by being burned at the stake, and still others were placed in almshouses intended to house the poor. Indeed, the first asylums were jails and almshouses where great abuse of the mentally ill occurred.2
The large numbers of people recognizable as mentally ill but who did not exhibit threatening behavior led to the realization in the mid-1300s that there needed to be hospitals to provide for their care and sustenance. One of the first and most notorious was the Priory of St. Mary of Bethlehem in London, which became the Bethlehem Royal Hospital. Over time, it became better known by the nickname of “Bedlam.” By the middle of the 16th century, Bethlehem Royal Hospital was entirely dedicated to caring for those suffering from serious mental illness. As leprosy became less prevalent in the early to mid-1500s, the asylums built to house lepers were also converted to be among the first lunatic asylums.3
In the 16th century, science and medicine were beginning to be explored in depth, and approaches to many aspects of life were changing as a result. It began to be understood that mentally ill people were suffering from some as yet unknown disease process. While asylums were established in Europe, these were places of terrible mistreatment. “Patients,” regardless of the manifestations of their mental illness—the quiet, morbidly depressed, the loud and delusional manic, and the violent—were held together in small, dank rooms and never released. Those who were uncooperative were beaten and chained to their beds. The period in which this type of treatment was the norm lasted for hundreds of years.4
Mental Illness in Early America
Serious mental illness (SMI) has also been a problem for Americans and American communities since our colonial beginnings. In the 1700s, most people with serious mental illness lived with family, which is similar to early mental health treatment in Europe. However, those not manageable at home often ended up as beggars on the street, unsheltered, or were placed in prison. As in Europe, early American colonialists used isolation and physical restraint as a common approach to those with auditory and visual hallucinations and delusions. As the number of people suffering from these mental illnesses increased, the first public and private psychiatric hospitals were built in the colonies in the late 1700s.
In the 1800s, there was a shift to what was termed “moral treatment” of the mentally ill. New asylums focused on the care—rather than the restraint—of those with serious mental illness. There was a belief that kindness could be curative. “Moral treatment” avoided the use of harsh physical restraints and forbade physical abuse of patients. When necessary for safety, gentler restraints such as straitjackets, hand-straps, and bed-straps could be utilized for the shortest periods of time possible. While these methods could be abused, there was awareness that such interventions substantially impacted individual freedom, and efforts were made to minimize these approaches.
In 1841, the Institute of Pennsylvania Hospital opened, and a physician named Thomas Kirkbride became the superintendent.5 Dr. Kirkbride developed a plan for architectural design of asylums that would house a maximum of 250 patients who would live in a building with a central core and long wings built to provide maximum access to sunshine and fresh air, while also focusing on privacy and comfort, and served wealthy clients with mental illness.6 This new hospital, dedicated to the moral treatment of the mentally ill, opened in 1859 and operated until 1997. This approach became a model for such facilities, and other similar hospitals for the mentally ill were built, but again, they mainly served families of means with loved ones needing such care, usually for life, as there were no effective medical approaches to mental illness at that time. In the 1850s and 1860s, Dorothea Dix advocated to state government officials for the same types of facilities to address the needs of the poor with mental illness in the United States.7 By the 1870s, nearly all states had at least one of these types of state hospitals funded with tax dollars.
Over time, these state hospitals, which were highly regarded for the environment they were able to provide to the severely mentally ill, shifted in terms of the types of patients being admitted. By the 1890s, there was a push to place the elderly with dementia into these psychiatric hospitals. The result was overcrowding and the loss of the therapeutic milieu.8 The decline of the state psychiatric hospitals continued into the 1900s. Overcrowding, low staff pay, long hours, and a shortage of doctors provided an environment in which abuse occurred.9 Serious abuse with harsh restraint and long-duration seclusion, as well as beatings of patients, went unnoticed by state officials. With the onset of World War II, state hospitals experienced a further loss of funding and a loss of staff causing conditions to worsen.10
The Vilification of Treatment and Rehabilitation
In 1946, one year after the end of World War II, Life magazine published an exposé on state hospitals, which included eye-opening photographs.11 This article details primitive, overcrowded, unhygienic living conditions and outdated and ineffective treatments, and this is portrayed from the vantage of individual stories. Americans, who had only recently learned of the Nazi atrocities in Europe, complete with photographic stories of the genocide that occurred there, were shocked to learn that such an abusive system existed within the United States. They saw disturbing similarities between the state hospital system and what occurred in Europe. This exposé advocated for people to support reform of the mental health system, better funding for mental health services, and research into these conditions and their treatment. The movement to close state hospitals and advocacy for the rights of the seriously mentally ill gained momentum and became a major force, leading to the closing and reduction in bed numbers for state hospitals nationwide.12
Pharmaceutical Idealism
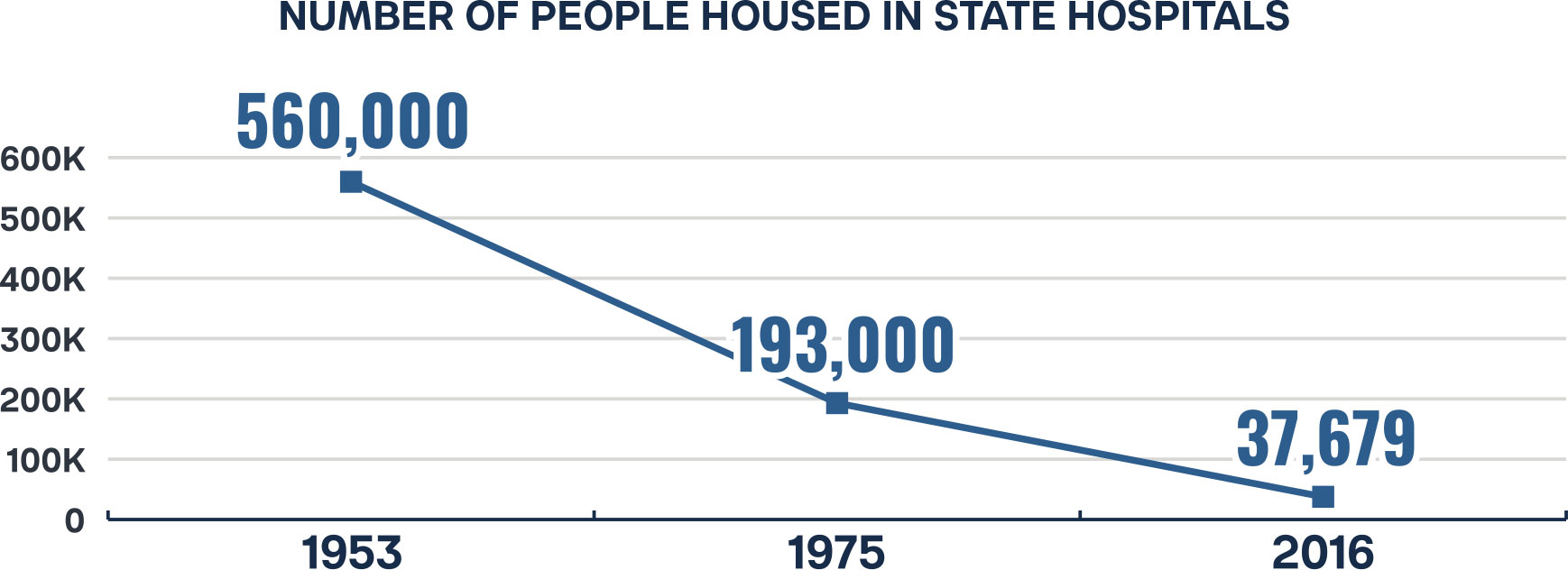
Pharmaceutical responses were also evolving with the discovery of chlorpromazine (Thorazine), a medication originally developed to address “surgical shock” and found to be a calming agent, leading to its use in the treatment of psychosis. Chlorpromazine was found to relieve hallucinations and delusions and the cognitive disorganization of schizophrenia, although it had little effect on the pervasive social withdrawal associated with the illness. Chlorpromazine was the first medication treatment found to be effective in the treatment of mental illness, and its use became widespread by the mid-1950s.13 This discovery was another major factor in the deinstitutionalization of thousands with psychotic disorders who had been living in state hospitals. Indeed, the highest numbers housed in state hospitals were reported to be 560,000 in 1953—a number which dropped to 193,000 by 1975,14 and further to 37,679 in 2016.15
Legislating Deinstitutionalization
The problem with the deinstitutionalization of hundreds of thousands of people with serious mental disorders is that simply discharging them, although they continue to experience severe symptoms, makes it impossible for them to take care of themselves. They cannot be expected to obtain and keep employment, housing, and financial resources necessary for survival. The intention of the United States—at least from a federal level—was made clear in the 1963 Community Mental Health Act, which funded the building and initial funding of Community Mental Health Centers across the country. These were meant to provide mental health services to all in need and make it possible for people previously institutionalized to live successfully in their communities.
The reality of what happened in the wake of this major legislation is a mixed story. Only about half of the planned community mental health centers were built, but 90 percent of state hospital beds were shuttered.16 This left a significant number of people with serious mental and substance use disorders who were not responsive to treatment (if they were able to find it), relegated to the streets, emergency departments, or jails and prisons. In 2013, USA Today reported that “The three largest mental health providers in the nation today are jails: Cook County in Illinois, Los Angeles County, and Rikers Island in New York.”17
People with serious mental illness would soon face more difficulties when discharged from state hospitals. In 1965, Medicaid-enabling legislation was signed into law. This legislation included the Institutions for Mental Diseases (IMD) exclusion, which prohibited Medicaid payments to any healthcare facility principally providing care for either mental or substance use disorders, and having more than 16 beds.18 This guaranteed that many people who were severely mentally ill or addicted would have no choice but to forego urgent care needed to address disabling symptoms requiring inpatient care or to wait excessive periods of time in an emergency department for a psychiatric bed to open somewhere.
In addition, the focus of Medicaid was on addressing physical illness, and, for outpatient care, this took the form of funding for a national system of Federally Qualified Health Centers (FQHCs). These programs, funded using a cost reimbursement formula, had the resources to provide high-quality care. The FQHC also traditionally provides treatment for mild to moderate mental illness and substance use disorders, but not for the most severe behavioral health conditions. This approach assured that those with lesser need would have access to mental health services, while the most severely ill languished. FQHCs generally lack the psychiatric expertise necessary to attend to the needs of the severely mentally ill or substance-abusing person.
Litigating Deinstitutionalization
Historically, the U.S. has permitted broad institutionalization under a “need for treatment” model. In the early 20th century, individuals could be committed indefinitely based on mental illness alone, often without judicial oversight. This changed shortly after the Life magazine exposé with the rise of the civil rights movement and deinstitutionalization in the 1960s and 1970s, which emphasized individual liberty and community-based care. President Kennedy’s Community Mental Health Act of 1963 started a cascade of events that led to the modern incarceration of the mentally ill.19 With the best of intentions, President Kennedy sought to reduce the number of mentally ill people confined in permanent care in psychiatric hospitals and focus on community-based support and pharmacology. He was easily swayed because of personal experience with his sister’s mental illness, but was unfortunately sold a promise of effective treatment that never came to fruition. Specifically, Kennedy’s act outlined longterm plans for community mental health centers while improving existing psychiatric facilities and services. However, behind the scenes, there was discord across psychology and psychiatry regarding the causes of mental illness—biology or social determinants of health, and the need for medicine and psychotherapy. Collectively, the psychiatry field came together to support the Community Mental Health Act while also focusing on the use of new psychotropic medicines, at the expense of funding state mental hospitals.20 The result was a funding crisis as federal subsidies were limited, and the states had few mechanisms to support the continued operations of state-run facilities without them.21
The federal deinstitutionalization movement, the result of what Kennedy started, began in full force in the 1970s. This was roughly at the same time as the infamous Martinson Report (1974),22 which called into question all penal institution-based rehabilitation efforts in the criminal justice system. This work, titled “What Works: Questions and Answers about Prison Reform,” was meant to advocate for community-based corrections, but was instead reinterpreted by politicians as “Nothing Works” for rehabilitation and ushered in the “get tough” era of criminal justice sentencing. Concurrently, the War on Drugs, War on Crime, and War on Poverty were occurring, which created a public fear of crime, drugs, and people deemed “different.” Largely thanks to President Nixon’s targeted use of the War on Drugs toward those involved with the civil rights movement, anti-war movement, and hippie movement, the way was paved for societal collateral damage, which had a major negative effect on the seriously mentally ill.23 Without supportive services, and in an environment of increasingly punitive political and public pressures, what emerged were three avenues for the seriously mentally ill who do not have the benefit of support networks (e.g., family) or money: homelessness, forensic hospital beds, or incarceration.
From a legal standpoint, the landmark U.S. Supreme Court case O’Connor v. Donaldson (1975)24 established that:
“A State cannot constitutionally confine a non-dangerous individual who is capable of surviving safely in freedom.”
This ruling effectively ended indefinite hospital institutionalization without proof of dangerousness, leading to the adoption of “dangerousness” standards across civil commitment statutes. This decision marked a legal shift: dangerousness became a constitutional requirement for civil commitment. While this seemingly preserved civil liberties, it also left a gap in care for individuals who were gravely ill but not actively dangerous. This gap has contributed to rising homelessness, incarceration, and repeat hospitalizations among people with untreated mental illness as they cycle through episodes of erratic behavior.25
Additionally, the Lake v. Cameron (1966)26 ruling emphasized the least restrictive alternative principle, further strengthening the need for narrow interpretations of dangerousness. While this ruling (born of the civil rights movement, new psychiatric medicines, and a growing belief in community-based care) successfully reduced the population of state psychiatric hospitals, it failed to build reasonable alternatives. As a result, many individuals with serious mental illness were displaced into prisons, hospital emergency departments, and the streets of American communities. For example, the state mental hospital census plunged from 560,000 in 1955 to only 216,000 by 1974 and approximately 100,000 by 1989.27 The displacement from state psychiatric hospitals to other areas has become more apparent as nationwide, the shortage of psychiatric beds remains acute.28 By 2016, analysts observed that U.S. correctional systems housed nearly 10 times as many people with serious mental illness as the combined total in psychiatric hospitals.29
Consequences of Deinstitutionalization
Figure 1 gives a grim picture of the movement of the severely mentally ill from state hospitals in the mid to late 1970s to the present day. Concomitantly, there is a significant rise in the number of people suffering from severe mental illness ending up in prisons and jails, with a similar, although not as dramatic, rise in the seriously mentally ill who are homeless.

As shown in Figure 1, jails and prisons have become de facto mental institutions in this country. Those with serious mental illness are often unable to recognize that they have a mental disorder and need treatment.30 This is a symptom of mental illness termed anosognosia. Such individuals frequently decompensate in their mental abilities to the point where they commit infractions of the law, leading to arrest, incarceration, and release without a requirement for treatment of mental and/or substance use disorders, causing this scenario to occur repeatedly.31 As a society, we have chosen to call this cycle a “civil right” rather than to humanely provide, and where necessary compel, mental health and substance abuse treatment.
Currently, there are 1,828,000 adults incarcerated in America.32 Approximately 20 percent of the jail population, estimated at 550,000, and 15 percent of the 1,071,000 inmates in state prisons are estimated to have a serious mental illness.33 If we use the Federal Register’s estimate for an average yearly cost of incarceration of $42,672, the cost of incarcerating the seriously mentally ill is over $13 billion every year.34
Modern-day civil commitment—also known as involuntary hospitalization—is a legal mechanism by which individuals may be detained and treated for mental illness or substance use disorders when deemed a risk to themselves or others.35 The threshold for such commitment hinges on the concept of dangerousness, a criterion fraught with historical ambiguity, legal scrutiny, and clinical complexity. The subjective nature of this standard makes it a complex intersection of law, psychiatry, and public ethics. Understanding dangerousness requires an exploration of how it has been defined, interpreted, and reformed throughout American legal and mental health history.
Conclusion
The history of mental illness in both Europe and the United States reveals a long and often troubling evolution of care, shaped by shifting beliefs, social attitudes, and legal frameworks. From early spiritual interpretations and brutal confinement to the emergence of moral treatment and state psychiatric hospitals, approaches to mental illness have alternated between neglect, abuse, and reform. The mid-20th century brought optimism through psychotropic medications and deinstitutionalization, yet the failure to establish adequate community-based supports has left many individuals with serious mental illness vulnerable to homelessness, incarceration, and repeated crises. Today, the intersection of law, psychiatry, and public policy continues to challenge society to balance civil liberties with humane, effective treatment, highlighting that the journey toward comprehensive mental health care remains incomplete.

Stay Informed
Sign up to receive updates about our fight for policies at the state level that restore liberty through transparency and accountability in American governance.