
Reducing Homelessness by Confronting Mental Illness and Substance Abuse




Issue Areas
Related Content
Introduction
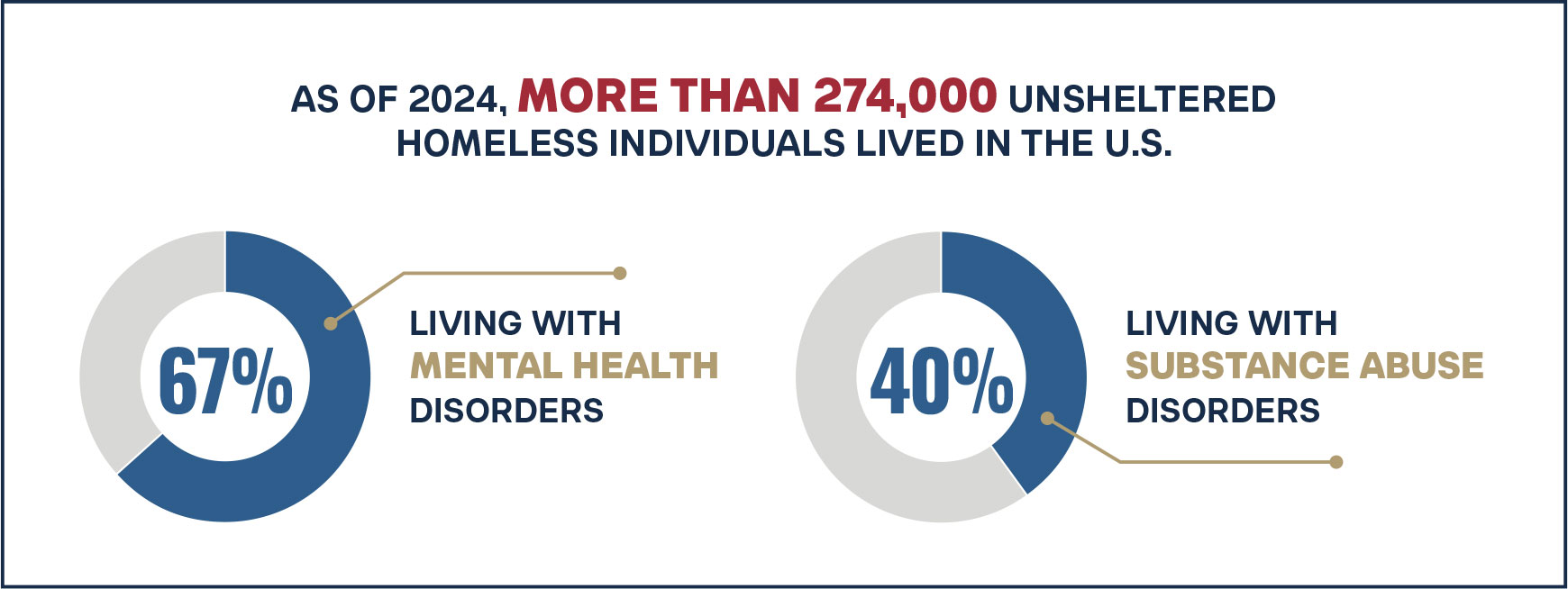
Homelessness in the United States has increasingly intersected with behavioral health challenges over the past five decades. As of 2024, more than 274,000 unsheltered homeless individuals lived in the U.S., with approximately 67 percent living with mental health disorders and more than 40 percent living with substance use disorders.1,2 In other words, as many as two-thirds of people experiencing homelessness suffer from a mental health disorder, a substance use disorder, or both. This reality underscores the urgent need for interventions that go beyond providing shelter to directly address behavioral health needs.
The roots of this crisis stretch back to the 1970s and 1980s, when the closure of psychiatric hospitals, the demolition of low-cost single-room housing, and the decriminalization of vagrancy and public drunkenness converged to push vulnerable individuals onto the streets. Since then, the profile of homelessness has shifted from transient populations to a far more complex cohort that includes individuals with severe, untreated psychiatric disorders and addictions. The result is a national homelessness crisis that is not only more visible but also increasingly resistant to simplistic solutions offered by Housing First ideologies. Skid rows continue to grow, providers are poorly resourced, and housing for the homeless fails to scale while being plagued by high rates of violence, poor maintenance, and high vacancy.3
Against this backdrop, the President’s Executive Order “Ending Crime and Disorder on America’s Streets” represents a significant shift in federal homelessness policy. The EO explicitly acknowledges the link between unsheltered homelessness and untreated behavioral health conditions such as mental illness and addiction. By emphasizing public safety alongside human welfare, the EO moves away from policies that frame homelessness solely as a housing problem. It also recognizes that organizations working to end homelessness must be held accountable for outcomes and, in doing so, acknowledges both the historical failure of Housing First providers to deliver acceptable outcomes and the promise a renewed focus on behavioral health holds for delivering better ones. This reframing marks a vital opportunity to realign federal strategy and policy with on-the-ground realities.
Policy Context
For decades, federal homelessness policy has been dominated by the Housing First approach, which became the preferred model under the Homeless Emergency Assistance and Rapid Transition to Housing (HEARTH) Act of 2009. First embraced under President Bush in 2000, Housing First lowered barriers to shelter by eliminating requirements that homeless individuals receive treatment, achieve sobriety, or participate in recovery programs before entering housing programs.4 While this approach made housing more accessible in the short term, it often neglected the psychiatric and addiction-related challenges that prevent many individuals from maintaining stability over time. The HEARTH Act, signed into law by President Obama, further solidified the shift away from a treatment-first to a housing-first approach.5 As a result, the homeless experience disproportionate mental illness and substance abuse, leading to a high mortality rate and an average life expectancy almost 30 years lower than that of the general population.6,7
Billions of dollars have been poured into this model, particularly in states like California, where between 2018 and 2021 alone, more than $25 billion was spent on homelessness initiatives. The outcomes, however, have been underwhelming. Despite substantial increases in federally subsidized permanent supportive housing and rapid rehousing units, unsheltered homelessness has continued to rise, particularly among those with serious behavioral health needs. Between 2023 and 2024, unsheltered homelessness across the nation increased by 18 percent. Federal spending to address homelessness was proposed to increase by 6 percent to $10.3 billion in 2024 for 771,480 homeless individuals.8,9,10 Compared with the 2024 budget for homelessness, the 2023 budget for homelessness was $9.71 billion for 653,104 homeless individuals.11,12 Without a significant change in policy, both the federal homelessness budget and the number of homeless individuals are likely to continue growing year after year.
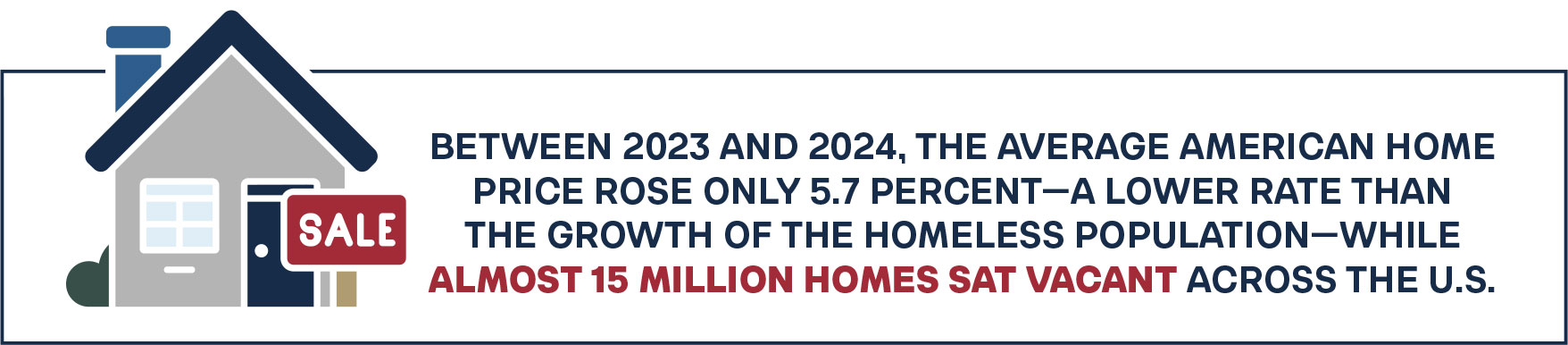
At its core, Housing First assumes that homelessness is primarily a housing supply issue. But this explanation is complicated by recent data: between 2023 and 2024, the average American home price rose only 5.7 percent—a lower rate than the growth of the homeless population—while almost 15 million homes sat vacant across the U.S.13,14 Florida, for instance, has both the nation’s fourth-largest homeless population (31,362) and the 5th-highest number of vacant homes (1.5 million), including in affordable areas where 17 of every 20 homes are valued under $200,000.15,16,17 This state of affairs challenges the often-heard argument by Housing First advocates that homelessness is caused by a lack of affordable housing. Instead, it indicates that homelessness persists even when affordable housing is available, which in turn suggests that widespread behavioral health and addiction challenges among homeless populations are to blame. Unless mental illness and addiction are addressed, housing subsidies alone will continue failing to generate lasting recovery or stability. Moreover, they will continue doing nothing to help the 36 percent of the total homeless population that are unsheltered, where serious mental illness and addiction are most concentrated.18,19
In addition to concerns about Housing First, barriers to the provision of treatment for both homeless persons and the general population are under scrutiny. Policy and law on issues such as civil commitment, involuntary treatment, Medicaid reimbursement for mental illness, and suitable settings that balance civil rights, community integration, and positive treatment outcomes are being reconsidered. Contemporary mental illness treatment policy has allowed the civil rights of the seriously mentally ill to preempt life-saving treatment and involuntary commitment. State civil commitment standards, the interpretation of the United States Supreme Court’s Olmstead v. L.C. decision, and state patient protection and advocacy agencies all present unnecessary barriers to civil commitment. The slogan adopted by many families of the seriously mentally ill is that their loved one “died untreated on the street with their rights fully intact.”
Reform Initiatives
In light of the failure of federal homelessness assistance programs to reduce homelessness, as well as the fact that a significant subpopulation of the unsheltered have serious mental illness or substance use disorders, several federal and state reform initiatives have been initiated. The following is a short summary of such reforms:
Homelessness Assistance Reforms
Changes to the federal Continuum of Care Program, especially involving the removal of prohibitions against participation in treatment, workforce, and other programs; outcome measures; and flexibility in housing types eligible to receive federal support.
Reducing Barriers to Treatment
Lowering thresholds for involuntary treatment, expanding the definition of dangerousness, and including substance use disorder as a qualifying condition for civil commitment proceedings are all being considered at the state level. In addition, clarifying the intent of the Supreme Court’s Olmstead decision will help ensure that people receive the help they need.
Reimagining Settings for Chronic Populations
Investing in treatment settings to expand the number and types of residential treatment options and provide pathways to increase or decrease treatment in response to outcomes or circumstances. This includes a return to and expansion of secure settings for the most severe cases.
Protection and Advocacy for Individuals with Mental Illness (PAIMI) Re-evaluation
The selection and empowerment of patient protection and advocacy organizations are being reevaluated to support efforts to increase access to treatment.
Pairing Housing and Treatment
Supportive and recovery-oriented communities are showing promise not only in reducing homelessness, but also in improving health outcomes among people with chronic conditions, serious mental illness, and addictions. Pairing treatment through programs like Certified Community Behavioral Health Clinics with housing and shelter options provides multiple benefits for homeless individuals and communities.
Enforcement of Public Spaces
Camping bans, drug-free homeless zones, and sanctioned camp areas are all measures directed at making public spaces safer. States and localities are implementing these tools and finding success.
Conclusion
The Cicero Institute has emphasized that ignoring behavioral health undercuts the effectiveness of homelessness interventions. Without requiring or facilitating treatment, many individuals cycle back into homelessness, incarceration, or emergency care. In contrast, approaches that integrate housing with evidence-based mental health and addiction treatment better support both individual recovery and community safety. Historically, treatment-first solutions to homelessness have sometimes been criticized as less effective.20 Housing First advocates have overreacted to such criticisms, dismissing treatment even where the evidence supports it. As a result, they have turned a blind eye to the very conditions that often lead to homelessness, especially chronically unsheltered homelessness, and the treatment requirements that can help remedy them.
Addressing homelessness without directly confronting the intertwined crises of mental illness and addiction has proven to be a failed strategy. The prevalence of severe mental illness and substance use among the homeless population—affecting well over two-thirds of those living unsheltered—means that interventions must prioritize treatment alongside housing. Yet for decades, federal policy under Housing First has advanced the opposite approach: subsidizing housing while requiring little to no engagement with mental health or recovery services, all while the homeless face greater threats of victimization and death.21
The consequences of this neglect are evident. Between 2013 and 2024, despite a more than 200 percent increase in the supply of permanent supportive housing, unsheltered homelessness has surged 28 percent nationwide, with particularly sharp increases among those with mental illn ess (27 percent) and substance use disorders (24 percent).22,23,24,25 This trend demonstrates that housing alone cannot resolve the crisis and that continued reliance on Housing First risks perpetuating cycles of instability, crime, and overdose deaths.

Homelessness is not solely a housing problem—it is fundamentally intertwined with behavioral health. Neglecting this dimension has left many unable to succeed in existing interventions and has contributed to persistent homelessness despite massive public investment. By aligning policy with the realities of mental illness and addiction, and by ensuring treatment access and accountability, federal and state governments can move toward sustainable solutions that reduce homelessness, improve public safety, and support recovery. Such a reorientation is not only necessary to reduce homelessness but also to restore safety, dignity, and order to America’s streets. The recent Executive Order signals that the era of housing-only solutions is coming to an end. The future of homelessness policy must embrace a recovery-centered model—one that integrates shelter with robust behavioral health services—to truly break the cycle of despair and create lasting change.

Stay Informed
Sign up to receive updates about our fight for policies at the state level that restore liberty through transparency and accountability in American governance.